Summary of article: Combined anterior-to-posterior and posterior-to-anterior approach to paranasal sinus surgery: an update. Schaefer SD, Li JC, Chan EK, Wu ZB, Branovan DI.Laryngoscope. 2006 Apr;116(4):509-13This article first reviews the historical development of FESS, from Wigand's postero-anterior approach (expose posterior ethmoids, open face of spehnoid, and retrograde ethmoidectomy) to the antero-posterior approach of Messerklinger & Stammberger (anterior ethmoidectomy followed by antegrade dissection posteriorly, extent determined by disease.) Kennedy's FESS is built on these antecedent techniques with the aim of 'reestablishing sinus drainage & mucosal recovery through restoration of obstructing sinus ostium and removal of devitalised mucous membrane or bone.'
The obvious advantage and disadvantage of the P-A approach is that
1. it avoids the skull base
2. surgery is excessive in cases of limited disease
As for the A-P approach:
1. surgery is selective and limited to pathologic sinus
2. there is potential for penetrating the posterio-inferiorly sloping skull base
The author's (Schaeffer) CAPS (combined approach to paranasal sinuses) is introduced and discussed. It is claimed that CAPS aims to 'bring together the salient features of the AP and PA approaches while observing the concept of functional endoscopic sinus surgery' and is therefore a 'minimally invasive surgery.. seeking the least disruption of form and function of the paranasal sinuses'
Key tenets of the combined approach are :
1. It is a 'disease-and-anatomy-oriented surgical approach'
2. It's goal is to 'conserve sinus anatomy'
3. Surgical principles utilizes 'anatomic relationships'
(It is disease-oriented in that surgery is targeted to 'relieve medically irreversibly obstruction of sinus outflow tracts' and it is anatomy-oriented in that anterior and posterior ethmoid sinuses are approached separately, in view that they are 'embryologically distinct structures... separated by the basal lamella of the middle turbinate.')
The key surgical principles include:
1. Complete uncinectomy necessary for anterior ethmoidectomy and prevent recurrence
2. Identification of MSO necessary to find plane of lamina papyracea
3. Anterograde (AP) dissection of anterior ethmoid cells up to basal lamella, retrograde (PA) dissection of posterior ethmoid cells
The authors' experience indicates that CAPS can be performed under local or general anesthesia, as permitted or tolerated. In this review of 2,344 patients, 'the overall complication rate was 3.4%. The minor complication rate was 2.6% (6 of 2,344 patients), and the major complication rate was 0.8% (2 of 2,344 patients).' Evidence that underscores how this 'hybrid technique' succesfully combines 'the conservation goals of the AP approach and anatomic virtues of the PA approach to ethmoidectomy.'
PubMed link








 'Heavner et al., in two animal studies, have demonstrated that exposure of the eustachean tube to simulated gastric content in rodents creates eustachean tube dysfunction. Velepic et al., in two separate studies, have demonstrated a strong correlation of otitis media and GERD. Using a 24-h double pH probe, they found that approximately 60% of the patients had pathologic GERD. In a 2002 study, Tasker et al. demonstrated that middle-ear effusions taken from 54 children contained pepsin/pepsinogen at concentrations up to 1000-fold greater than those in serum 83% of the time. These data suggest that the reflux of gastric juices could be a major cause for otitis media with effusion in children. The link between otitis media with effusion and pharyngeal reflux was further strengthened in a 2004 study by Keles et al. This dual-probe pH study demonstrated that 48% of the children with chronic otitis media effusion had GERD and 64% of the children had pharyngeal reflux. This study suggests that pharyngeal reflux may play an important role in the causes of chronic otitis media with effusion and also that standard single-channel pH probes evaluating for gastroesphageal reflux frequently will miss pharyngeal reflux.'
'Heavner et al., in two animal studies, have demonstrated that exposure of the eustachean tube to simulated gastric content in rodents creates eustachean tube dysfunction. Velepic et al., in two separate studies, have demonstrated a strong correlation of otitis media and GERD. Using a 24-h double pH probe, they found that approximately 60% of the patients had pathologic GERD. In a 2002 study, Tasker et al. demonstrated that middle-ear effusions taken from 54 children contained pepsin/pepsinogen at concentrations up to 1000-fold greater than those in serum 83% of the time. These data suggest that the reflux of gastric juices could be a major cause for otitis media with effusion in children. The link between otitis media with effusion and pharyngeal reflux was further strengthened in a 2004 study by Keles et al. This dual-probe pH study demonstrated that 48% of the children with chronic otitis media effusion had GERD and 64% of the children had pharyngeal reflux. This study suggests that pharyngeal reflux may play an important role in the causes of chronic otitis media with effusion and also that standard single-channel pH probes evaluating for gastroesphageal reflux frequently will miss pharyngeal reflux.' Should we blame everything on GERD? The above discussion, excerpted from
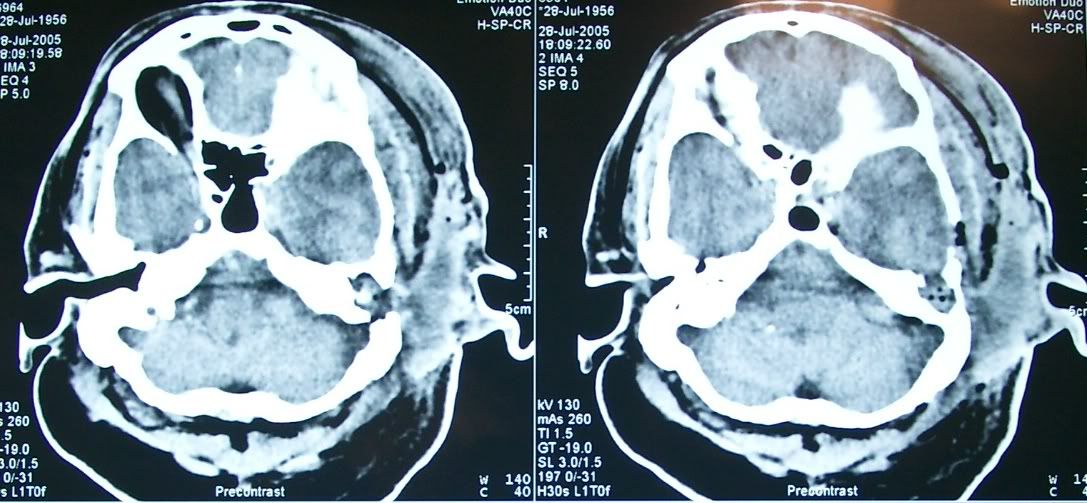
Should we blame everything on GERD? The above discussion, excerpted from 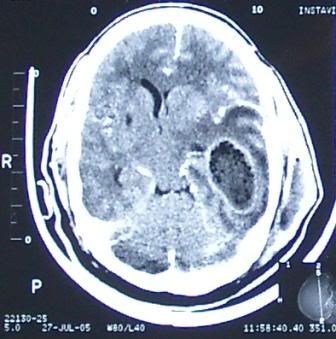 A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.
A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.