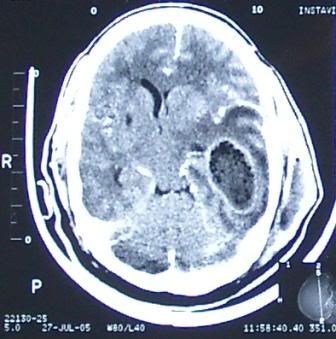
 A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.
A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.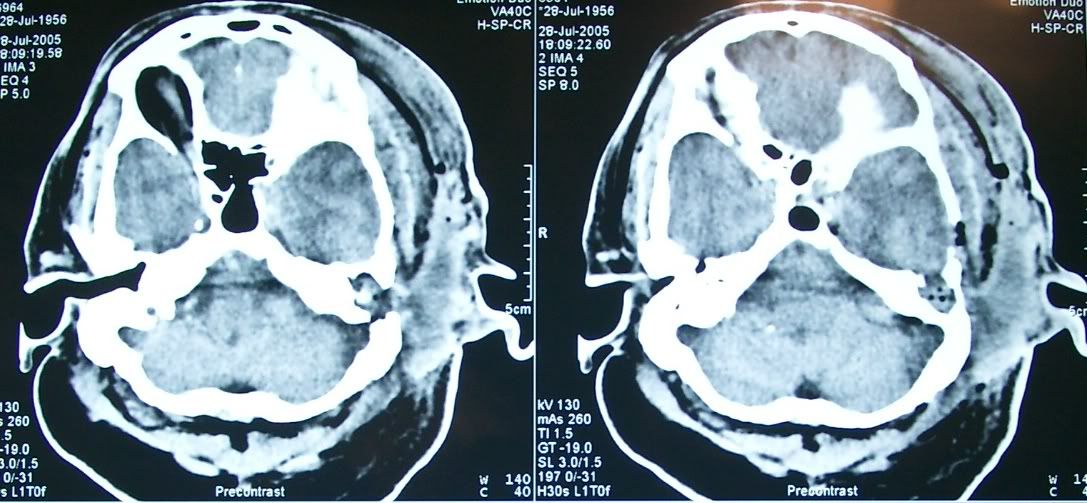
The history, however, was not quite so convincing. He had no history of chronic ear discharge, and was not diabetic. The only lead was one experience of external ear infection 3 months ago after he traumatised his ear canal by overenthusiastic cleaning. Examination would show an external canal filled with pus, a sagging posterosuperior meatal wall, a soft and fluctuant postauricular region and a discharging sinus.


I proceeded to perform a mastoid exploration/cortical mastoidectomy but to my surprise found only a sclerotic mastoid and no foci of disease at all. Drilling was carried all the way down to the bony defect where dura is clearly seen. No pus, granulation, or cholesteatomas found.
So where was the foci of infection? How did an abscess of such magnitude, with such extensive destruction of bone come about? We are hoping a HRCT will give us more clues. Could this be a skull base osteomyelitis secondary to otitis externa?


No comments:
Post a Comment