'Pneumatic otoscopy should be used to diagnose middle ear effusion. Clearance of OME may be prolonged in children with craniofacial abnormalities. Antibiotics provide a small short-term increase in the resolution of OME and may be warranted in children with coexisting SNHL and OME for 4 to 6 weeks. If OME persists for 8 to 12 weeks, bilateral myringotomy and tube placement (BM&T) with short-term tubes will improve hearing and help resolve OME. AOM in children less than 2 years of age should be treated with a 10-day course of antibiotics. Prophylactic antibiotics may be useful in avoiding tube placement in children less than 2 years of age with recurrent AOM. BM&T with short-term tubes are recommended if recurrent AOM persists. Pneumococcal vaccination can decrease episodes of AOM by 6 to 7%.'
Above are the recommendations based on a meta-analytic study by Westerberg BD, et al. in J Otolaryngol. 2005 Aug;34 Suppl 2:S64-9.
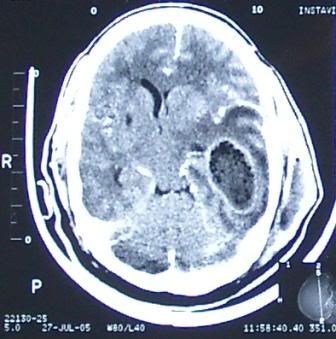 A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.
A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.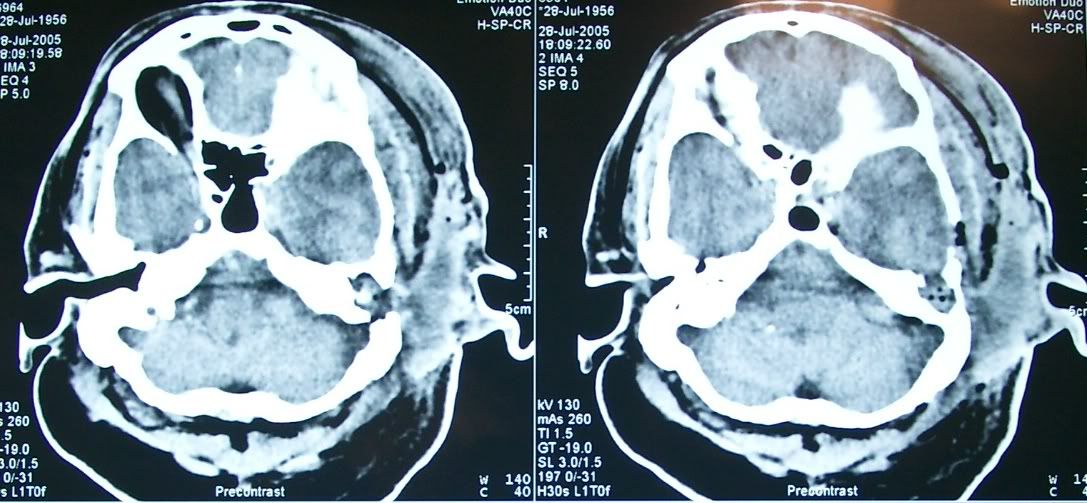


Q1: Skin Lesion
17 years ago

