by Y.Y.Yap, MD
Our understanding of rhinosinusitis and how we can best treat this ambiguous condition is in rapid evolution.
Fungal etiology for RSS
First off we have
Gosepath J and Mann WJ. take a closer look at the role of fungi role in initiating and maintaining CRSS. While fungi are ubiquitously present in ALL, an immunologic sensitization in RSS patients is evidenced by specific cytokine production in blood-derived lymphocytes not found in controls.
Sasama J, et.al also supports this theory showing from literature that eosinophilic inflammation in the nasal mucosa seems to be a specific reaction to certain molds in the nasal and paranasal cavities. Hence the shift from a bacteria-driven etiology to a fungal based one for RSS. It's implications for research and treatment is pressing and is reviewed in these articles. As though to dispel all doubt,
Ponikau JU, et.al boldy instituted a clinical trial and showed that intranasal amphotericin B reduces inflammatory mucosal thickening on both CT scan and nasal endoscopy and decreases the levels of intranasal markers for eosinophilic inflammation in patients with CRS.
Recurrent Rhinosinusitis - something different?
Bhattacharyya N, Lee KH. try to distinguish Chronic Recurrent (CRRSS) from Chronic Persistent Rhinosinusitis (CPRSS) by looking at a distinct group of patients who have symptom free periods between at least 4 episodes of RSS symptoms a year. Interestingly the chronic recurrents (CRRSS) seem to suffer more, require more antibiotics and miss work more than the chronic persistents.
FESS for children?
Lieser JD, Derkay CS review the role of FESS in children. Present consensus for FESS in children are 'when maximal medical therapy, adenoidectomy, and culture-directed systemic antibiotics have all failed with persistence of sinonasal disease, when anatomic abnormalities predispose to chronic rhinosinusitis by obstructing normal sinonasal drainage pathways, in sinonasal polyposis to facilitate application of topical steroids', among others. The debate for the best timing for surgery and the fine balance between interfering with facial growth vs. quality of life continues.
No limits!
The greats have spoken!
Cohen NA and Kennedy DW. have come forward to defend a larger role for the endoscopic surgeon, stating: 'Endoscopic sinus surgery is no longer exclusively for the management of chronic rhinosinusitis and nasal polyposis. Sinonasal malignancies, as well as anterior skull base lesions have become part of the rhinologist's responsibility. Furthermore, selective lesions managed through traditional craniotomies may now be accessed via trans-sinonasal transcranial endoscopic routes.' They attribute this increased scope, safety and efficacy to advancements in imaging technology including image acquisition, three-dimensional reconstruction, stereotactic navigation, and CT-MRI fusion.
Rapid steps forward are being made on the basic science, pharmacotherapeutics and surgical fronts in rhinology. The future is bright!
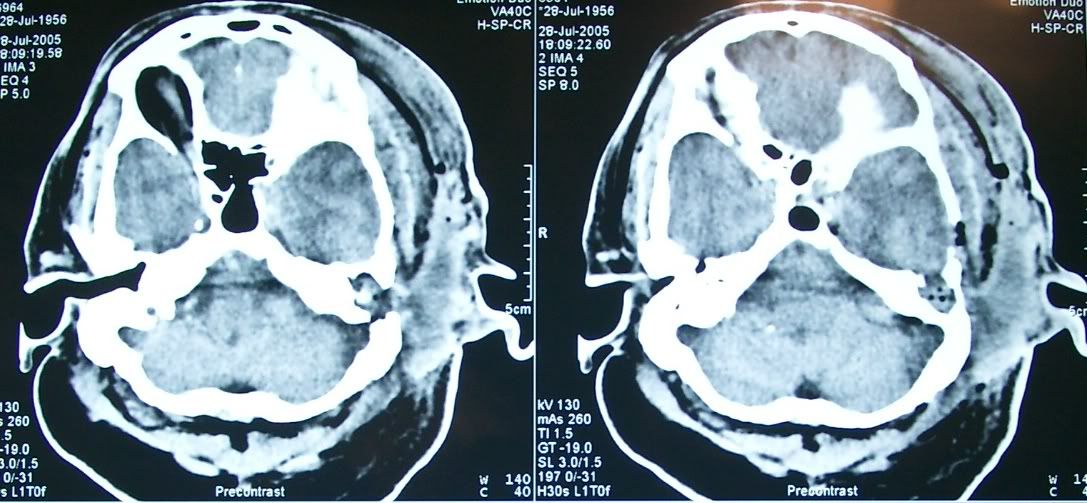
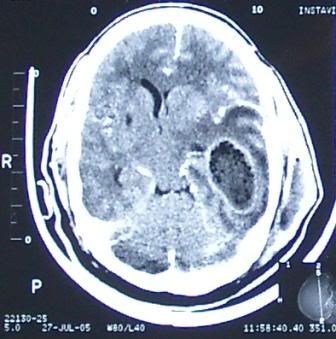 A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.
A 55yr-old man had craniectomy and drainage for a huge intracranial temporal lobe abscess and an ipsilateral extracranial temporal abscess as seen in this CT scan. He was referred to ENT for clearance of a possible foci of infection from the mastoid or middle ear which would seem to be the case from the 2nd image presented here. A large area of erosion is seen in the mastoid, communicating with the middle fossa as well as the temporal space.